About a decade ago, Beverly Rzigalinski, a molecular biologist now at Virginia College of Osteopathic Medicine, was asked by a colleague to look into nanoparticles. “Nanoparticles? Yuck,” she thought. She off-handedly told a student to throw them on some neurons growing in the lab and take notes on what happened. She had no hope for the experiment, sure the nanoparticles would kill all the neurons, but at least she could say she tried.
Rzigalinski was given cerium oxide nanoparticles to work with, ten-nanometer wide particles derived from a rare earth metal. (Human hair, by comparison, is 100,000 nanometers wide.) No one had looked at their biological applications, and Rzigalinski was not particularly impressed with their résumé. Cerium oxide nanoparticles’ listed industrial uses included glass polishing and fuel combustion, nothing that seemed promising for neuroscience.
A month and a half later, Rzigalinski noticed the dishes still sitting in the lab’s incubator. She marched straight over to the student, launching into a lecture about not wasting expensive resources on cells that were surely long dead. (Neurons in the lab typically stayed alive for only three weeks.) But the student assured her the cells treated with nanoparticles were still alive. Skeptically, she peered into the microscope and was surprised to find living, flourishing neurons. Rzigalinski has been studying nanoparticles ever since.
Other neuroscientists are joining her, taking advantage of nanoparticles’ unique properties to identify new therapies, shuttle existing therapies into the brain, and examine the brain on a level and depth never before possible.
Recyclable Antioxidants
When treated with cerium oxide particles, Rzigalinski’s neurons survived for up to six months, nine times longer than usual. Cerium oxide nanoparticles may extend life in this way by neutralizing free radicals, unpaired electrons that are highly reactive and can damage DNA. The body’s defenses against free radicals may wear down with time; aging may be due in part to free radicals slowly accumulating unchecked.
Damage induced by free radicals also contributes to a number of neurological diseases. Rzigalinski’s work is revealing how cerium oxide nanoparticles can prevent or reverse this destruction as well. Treating mouse models of Parkinson’s disease with cerium oxide particles rescued the loss of dopaminergic cells, the death of which leads to the disease’s characteristic tremors and slow shuffling gait. Cerium oxide nanoparticles also seemed to halt the free radical-triggered cascade of damage that typically follows traumatic brain injury; after injury, nanoparticle-treated mice had fewer signs of free radical damage and better memories compared to control-treated mice. Finally, when flies were administered nanoparticles following a stroke (in a timeframe analogous to receiving treatment upon arrival to a hospital), the treated flies not only lived longer but also had improved performance on fly-specific tasks, like quickly buzzing to the top of the cage.
Antioxidants like vitamins C and E also sop up free radicals, but each antioxidant molecule only destroys one free radical. As Rzigalinski points out, the advantage of cerium oxide nanoparticles is that, “These nanoparticles are regenerative, so they’ll scavenge thousands, or hundreds of thousands, of free radicals.” Cerium oxide nanoparticles neutralize free radicals by snatching the electrons, shuffling them around, and eventually depositing them as water, restoring the nanoparticles to their original state, ready to abolish more free radicals. This recycling means the nanoparticles will continue working after a single dose. Rzigalinski found nanoparticles present as long as six months after injection in mice and, crucially, toxicity has not been an issue, since the dosage is so low. Single doses, or even low doses, can both prevent harmful side effects and keep costs down.
Cerium oxide nanoparticles are effective because, after injection, they immediately get coated with proteins that help carry them into the heart, lungs, and brain—where they need to be to slash disease-causing free radicals. Not all drugs are so lucky.
Trojan Horses
The trouble with treating brain diseases is the brain exists in a separate world, sealed off from the rest of the body. Cells are tightly packed around the brain’s blood vessels, forming the blood brain barrier, a heavily guarded barricade separating the blood and its contents from the brain and spinal cord. This security system works to keep any bacterial infections and toxins in the blood from getting into the ultrasensitive brain. If small or fat-soluble enough, certain approved entities—like water, gases, alcohol, and some hormones—can leak across the border. Larger molecules require exclusive receptors to allow them through, a unique key that unlocks a particular door and grants them access.
While creating an extra level of protection from diseases outside the brain, the blood brain barrier causes trouble for trying to solve diseases within the brain. It’s a notorious nemesis of drug development, preventing an estimated 98% of potential treatments from getting in. Tomas Skrinskas of Precision NanoSystems—a biotechnology company specializing in delivering materials to cells—lamented, “The blood-brain barrier is probably the trickiest [challenge] there is.”
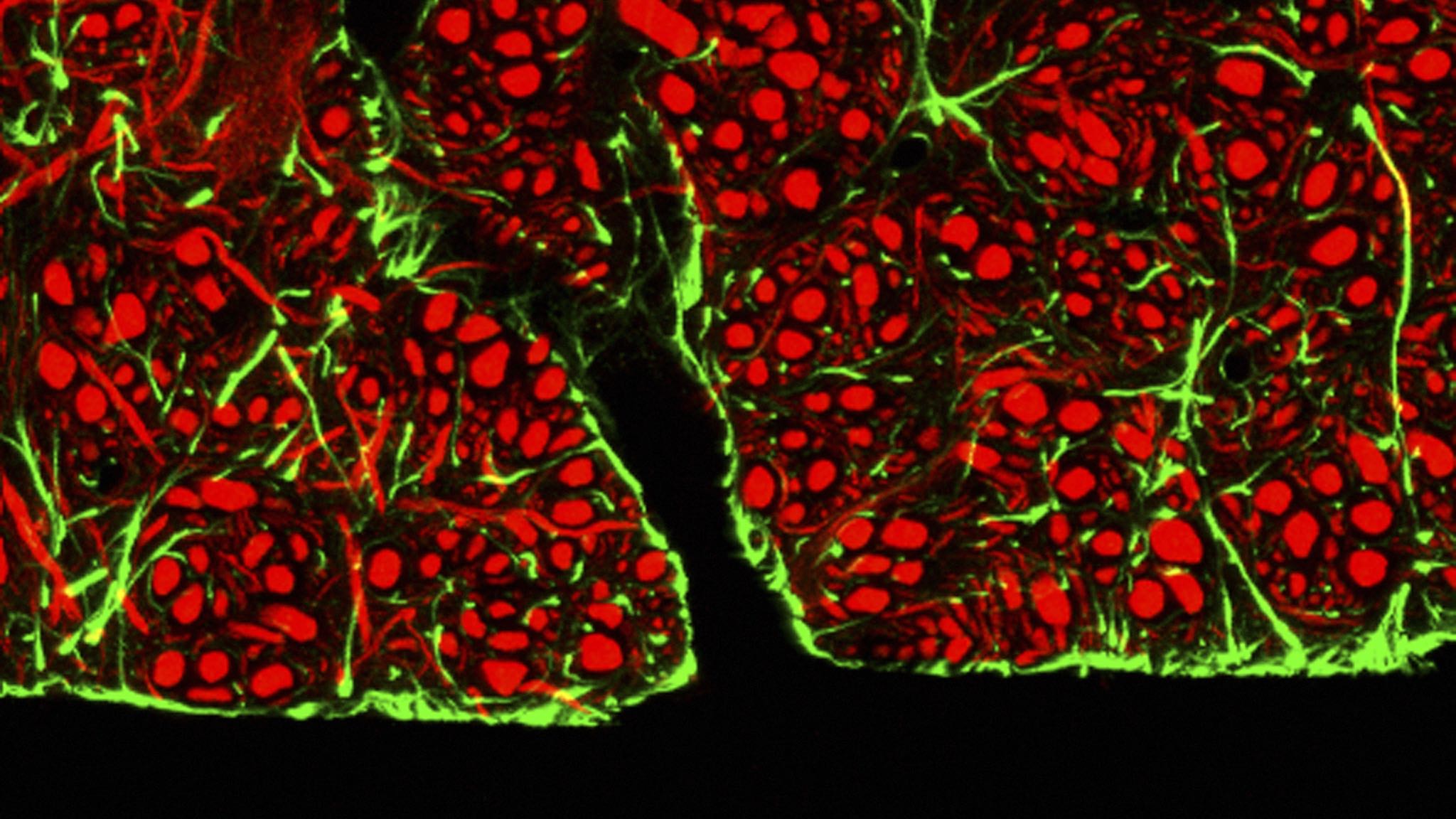
In this image of the blood-brain barrier, green-stained glial cells surround the blood vessels (seen here in black), providing support for red-stained neurons.
To overcome this hurdle, one current solution involves flooding the blood with drugs, hoping a small proportion passes through by sheer force of will or strength in numbers. But ingesting lots of drugs can trigger nasty side effects elsewhere in the body. Another way to crack through the defenses is to hack into systems already in place for transporting small molecules. Enter nanoparticles.
While some nanoparticles act as treatments, others play the role of Trojan horse: they pretend to be ordinary, recognized molecules, gain access through special receptors, and sneak the drugs with them as they pass through the restricted entry gates. Nate Vinzant, an undergraduate in Gina Forster’s lab at the University of South Dakota, is using iron oxide to smuggle anti-anxiety drugs into the brain.
When injected directly into the brain, antisauvagine decreases anxiety in rats. However, direct injection into the brain isn’t a feasible treatment option for humans and antisauvagine is incapable of passing from the blood to the brain on its own. To sneak it in, Vinzant attached antisauvagine to iron oxide nanoparticles, which are regularly taken into the brain via specific receptors. When hitched to iron, antisauvagine goes along for the ride because “the brain thinks it’s iron,” Vinzant says. Indeed, typically anxious rats given iron-bound antisauvagine displayed less signs of stress than untreated rats, confirming that the drug made its way from the injection site in the abdomen, through the blood, and across the barrier.
More than just a boon for anxiety treatment, this research is a proof of principle. Other drugs can be tethered to nanoparticles like iron and use the same uptake mechanism.
Remote Controls
In addition to improving treatments, nanoparticles can also help researchers understand diseases and the brain in general. President Obama’s BRAIN Initiative, a program aiming to map the neurons and connections within the human brain, is initially focused on the development of novel technologies that may lead to future breakthroughs. This fall, Sarah Stanley, a post-doctoral researcher in Jeffrey Friedman’s lab at Rockefeller University, received one of the initiative’s first grants to develop technology that uses nanoparticles to control neurons.
Stanley’s goal is to examine a diffuse network of neurons distributed throughout the brain. “We were really looking for a way of remotely modulating cells,” Stanley explains, but existing tools weren’t able to go deep or dispersed enough. For example, one popular new technique known as optogenetics, which uses light to activate neurons, wouldn’t work for Stanley’s project because light can’t penetrate very far into tissue. Another method involving uniquely designed drugs and receptors can’t be quickly turned on and off. So Stanley turned to nanoparticles.
Ferritin nanoparticles bind and store iron, and Stanley genetically tweaked the nanoparticles to also associate with a temperature-sensitive channel. When the channel is heated, it opens, leading to the activation of certain genes.
To generate heat, she used radio waves. Unlike light, radio waves freely penetrate tissue. They hit the ferritin nanoparticle, heating the iron core. The hot iron then heats the associated channel, causing it to open. Stanley tested the system by linking it to the production of insulin; when the radio waves heated the iron, the channel opened and the insulin gene was turned on, leading to a measurable increase in insulin. The nanoparticle is “basically acting as a sensor for radio waves,” says Stanley. It’s “transducing what would be entirely innocuous signals into enough energy to open the channel.”
To optimize the system, Stanley first tested it in liver and stem cells of mice, but she is now moving into mouse neurons, intending to turn them on and off with her nanoparticle remote control. The radio waves’ penetration should allow researchers to use this technique to manipulate cells that are both deep and spread throughout the brain. “This tool will allow us to be able to modulate any cells in any [central nervous system] region at the same time in a freely moving mouse,” Stanley notes.
For now, remotely controlling neurons in this way will only be used in research to discover more about these deep or dispersed networks. But eventually, it could potentially be combined with gene therapy to fine-tune protein levels. For example, in diseases with a mutated or dysfunctional gene, like Rett Syndrome, a developmental disorder causing movement and communication difficulties, gene therapy aims to replace the defective gene. Adding a functional gene isn’t always enough, however, as it must be adjusted to produce the appropriate amount of protein. Controlling the gene with radio waves and nanoparticles would allow doctors to carefully tweak the protein production.
Although that’s a long way off, nanoparticles are claiming their spot in the future of neuroscience. In a press conference on innovative technologies at November’s Society for Neuroscience Conference in Washington, D.C., David Van Essen, a neuroscientist at Washington University in St. Louis, indirectly praised Stanley’s project. “It was really exciting to see earlier this fall that the [National Institutes of Health] has awarded about 50 new grants for some amazing, innovative ideas.” He then went on to introduce Rzigalinski’s research on Parkinson’s disease, mentioning how nanotechnology is a new tool providing hope for reversing devastating diseases.
Neuroscientists may need to temper their excitement, however. Clinical trials for cancer treatments have stalled as some nanoparticles—including iron—have been found to generate free radicals, which can trigger cell death. But a compromise may be possible: iron nanoparticles are also being studied to enhance magnetic resonance imaging (MRI) signals and toxicity doesn’t seem to be an issue so long as the doses are kept low. If the drugs the nanoparticles carry with them are powerful enough, lower doses can be used and harmful side effects prevented.
So far, cerium oxide nanoparticles have avoided this issue, but their relentless crusade against free radicals may lead to a different problem: free radicals are crucial to certain cellular processes, including the regulation of blood pressure and function of the immune system. The question of how much free radical scavenging is too much remains to be answered. But, considering the elevated levels of free radicals in disease, perhaps the nanoparticles will have their hands full lowering levels to a healthy range, let alone reducing them enough to cause trouble.
It’s still too early to know whether nanoparticles will usher in a new wave of clinical treatments, but to many researchers, it’s clear that they show great promise. Rzigalinski, for example, has long since apologized to her student for her disbelieving rant. Small as they may be, nanoparticles have the ability to take on Goliath-sized tasks, bringing researchers deep inside the brain, past its defenses, ready to fight destructive forces in new ways.
If you’ve been diagnosed with fibromyalgia or are a caregiver to a loved one who’s suffering, you know how hard it is to physically and emotionally manage this condition. But there are treatments that can help. Get expert advice to ease symptoms and 5 tips to help soften the burden on caretakers…
Your body aches and you feel exhausted, yet you’re unable to sleep.
“Basically, you blew a fuse,” says internist Jacob Teitelbaum, M.D., medical director of the Fibromyalgia and Fatigue Centers and author of From Fatigued to Fantastic.
“Fibromyalgia represents an energy crisis,” says Dr. Teitelbaum, who suffers from the condition. “You’re spending more energy than you can make.”
If you’re wondering why or how you developed the disorder, don’t expect an easy answer. Fibromyalgia may run in some families and often follows infections or physical or emotional trauma. Or it appears for no reason at all. Women are 4-7 times more likely to have it than men, but the reasons are unclear.
Emotionally, you may be feeling confused, afraid and angry when neither you nor your doctor knows what’s happening to your body. In fact, your physician may even tell you there’s no medical problem and refer you to a psychotherapist.
“You may see eight doctors before you know what you have,” Dr. Teitelbaum says. “So you and your family may be given the impression that you’re crazy.”
It took Patricia Stephens, 62, author of Reversing Chronic Disease: A Journey Back to Health, 7 years before doctors put a name to her symptoms.
“I felt anxiety and fear,” Stephens says. “I was afraid of losing my job as a teacher, that I couldn’t raise my children or keep my marriage together, and that I would lose purpose and productivity.”Researchers are investigating hormones, immune system differences, brain chemistry and genetics for answers.
Because sufferers are especially sensitive to physical pain, they suspect that nervous-system problems may be a culprit.
Fibromyalgia pain generally targets 18 points on both sides of the body where pressure causes tenderness.
If sensitivity lasts at least three months in 11 out of 18 pressure points or muscle locations, you may have fibromyalgia, according to the American College of Rheumatology.
Making matters more confusing, fibromyalgia sufferers may also be diagnosed with other conditions, including irritable bowel syndrome, a gastrointestinal disorder characterized by either constipation or diarrhea; headaches; and/or temporomandibular joint syndrome (TMJ), which is inflammation of the jaw joint.
There are steps you can take to ease symptoms. Dr. Teitelbaum recommends a regimen he calls “SHINE”:
Sleep.For a better night’s rest, keep the bedroom at 65°F; take a hot bath before sleep to relax your muscles; and spray pillows with lavender oil, which helps promote sleep, he advises. Take 75-150 milligrams of magnesium, a natural relaxant, before bed. And avoid caffeine. Aim for 8-9 hours of shut-eye a night.
Hormones. Ask your doctor to test you for a possible hormone deficiency.
Infections.Lack of sleep may raise your vulnerability to viral or yeast infections. If you’re sick, see your doctor for treatment right away.
Nutritional supplements.Ask your doctor to test your vitamin levels, and take supplements as needed.
Exercise.Try yoga. Women with fibromyalgia who practiced yoga for eight weeks had a 24% pain reduction, 30% fatigue reduction and 42% depression reduction, according to a 2010 study at Oregon Health & Science University.
Also, consider having a massage. This may sound masochistic, given your sensitivity to pressure. However, fibromyalgia patients who got 30-minute massages twice weekly for five weeks slept longer with decreased restlessness during the night and suffered less anxiety and depression, according to a researchers at the University of Miami School of Medicine. They also registered lower levels of substance P, a neurotransmitter that raises pain sensitivity, which is often 2-3 times higher in fibromyalgia sufferers than people without the disorder.
Education, Exercise and Self-Management Conventional treatments typically address pain and sleeplessness. In 2007, pregabalin, an anti-seizure drug usually used to treat epilepsy, was the first drug approved to treat the physical pain of fibromyalgia.
Researchers believe the drug works by minimizing neuron transmissions that affect pain nerve signals.
Your doctor may prescribe duloxetine or milnacipran. These are antidepressants that increase brain chemicals to calm pain signals.
Besides one of these medications, your doctor also may suggest nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen to ease pain and stiffness.
But even if you take medications, you may still feel achy and fatigued — and frustrated that you’re not 100%.
“Having fibromyalgia can increase the risk of depression and anxiety,” says geriatric psychiatrist William Uffner, M.D., medical director for the Older Adult Program at Friends Hospital in Philadelphia.While being treated for fibromyalgia, continue with self-care steps, including the SHINE regimen.
Here are additional steps that can help:
Assess your mood. If you’re a grouch when you’re hungry, you may be low on cortisol, an adrenal stress hormone, says Dr. Teitelbaum. A holistic physician can check cortisol levels and perhaps prescribe a very low dose of cortisol. Go to the American Board of Integrative Holistic Medicine website for a list of board-certified holistic physicians.
Record your sleep. Sleep disturbances may be caused by sleep apnea, a condition in which breathing is interrupted, or restless-leg syndrome, which causes involuntary leg movements. Dr. Teitelbaum suggests videotaping yourself while sleeping: If your legs are twitching or you stop breathing periodically, see a sleep specialist.
Supplement your energy. Dr. Teitelbaum recommends taking ribose, a nutrient involved in energy production, to raise energy levels. “Studies show that patients’ energy increased 61% after three weeks, and sleep improved,” he says. His suggested dose is 5 grams three times a day for three weeks.
A recent breakthrough is the discovery of a new retrovirus, xenotropic murine leukemia virus-related virus (XMRV), found in most people with chronic fatigue syndrome (CFS).
“Within a year or two, there will be a test for CFS, which tends to overlap with fibromyalgia,” Dr. Teitelbaum predicts.
Though the link between CFS and fibromyalgia hasn’t been determined, the conditions may share a common cause, which is why the discovery of the virus is important. Researchers suspect that XMRV may lie behind other illnesses too.
A Vital Part of Caregiving As a caregiver, you may feel stressed and tired as you take on more responsibilities. You may also start to question whether your loved one is actually ill.
“You want to support your loved one, but you’re struggling with the extra load,” Dr. Teitelbaum says.Steps you can take:
Offer support. Your loved one already feels alone — and maybe foolish, for having an illness their doctor isn’t validating. “The No. 1 thing patients need to know is that you love and accept them,” Dr. Teitelbaum says.
Educate yourself. Learning about fibromyalgia can help you understand what your loved one is going through.
Avoid burnout. Learn to say “no” sometimes, says Dr. Teitelbaum. “Otherwise, you’ll be useless to the person with the disease. Or you’ll get sick yourself.”
Reserve some independence. Continue to do things you love apart from your loved one: hobbies, meeting up with friends, exercise. This will help you focus on the parts of your life that are going well, Dr. Uffner says.
Get support. Ask your doctor to refer you to a caregiver support group.By Dorothy Foltz-Gray
Considered a disorder, fibromyalgia consists of pervasive musculoskeletal pain, accompanied by memory and mood issues, fatigue and sleep problems, according to the Mayo Clinic.
Achy Body Triggers
There are many achy body triggers, and the weather is a big one. Barometric pressure is the measure of weight exerted by the air surrounding us. Right before a storm, barometric pressure drops, and this activates aches and pains.
The same goes for humidity. Humidity measures the amount of water vapor in the air. When it is low, patients are more likely to have a headache and suffer aching muscles and joints. Even being out in the wind can aggravate symptoms.
A Mystery
Doctors don’t know what causes fibromyalgia specifically, the National Institutes of Health reports.
However, the Mayo Clinic notes women are far more likely than men to acquire this disorder. Those suffering from fibromyalgia are more apt to have TMJ (temporomandibular joint pain), anxiety, depression and irritable bowel syndrome.
The Mayo Clinic notes that researchers believe this disorder makes people feel pain more profoundly than those who don’t have the condition. This is believed to happen because of the way the brain processes pain signals when you have fibromyalgia.
No Magical Cure for an Achy Body
So far, fibromyalgia is not curable, explains the Mayo Clinic. That said, there are medicines available on the market that have helped some sufferers.
There are increasing documented cases showing that IV Ketamine Infusions are very effective in the treatment of Fibromyalgia.
How To Treat the Aches?
The Mayo clinic recommends getting massages by a professional, if possible. Getting a back rub from a family member or friend runs a close second. They also say that there are over-the-counter inflammatory medications that dull the pain. Before taking them, check in with your physician.
Yoga reduces pain and helps maintain flexibility. Being outside on a warm, dry, sunny day is very therapeutic. Soaking in a hot bubble bath filled with Epsom salts relieves aches and pains too.
When under stress and the patient’s achy body demands attention, yoga and deep-breathing exercises go-to solutions. They lessen physical and mental pain and angst. Connie Ludtke, R.N., a Mayo Clinic expert, agrees that learning to relax is very important in coping with fibromyalgia.
When it’s cold and damp outside, dress in layers, wearing tights aggravates Fibromyalgia symptoms.
Can surgery patients eat their way to less postoperative pain?
A recent study by French researchers suggests that a diet low in polyamines can reduce pain after spinal surgery, with few side effects.
“There have been some data to show that a polyamine-deficient diet decreased pain in rats,” said Jean-Pierre C. Estebe, MD, PhD, professor of anesthesiology at University Hospital of Rennes in Rennes, France, who led the latest work. “This effect is likely due to polyamine’s modulation of the N-methyl-D-aspartate (NMDA) receptors. But no data are available on the potential efficacy of a polyamine-deficient diet on perioperative pain, so we decided to undertake a prospective, randomized trial with chronic pain patients with high levels of pain.”
Dr. Estebe and his colleagues enrolled 64 spine surgery patients into the study. Patients were randomized to one of two diets. Those on the polyamine-deficient diet ate a low-polyamine breakfast supplemented with six 250-mL low-polyamine drinks per day.
“Just to drink that, they received around 10,000 kcal per day,” Dr. Estebe said. Controls had a partial polyamine-deficient diet comprising two of the drinks each day plus regular food. “The study group received less than 10 micromoles per day of polyamine, while controls received an average of more than 400 micromoles per day,” Dr. Estebe explained.
The diets were initiated seven days before spine surgery and continued until five days after the procedure. The primary end point was pain at rest and with motion. Researchers also monitored compliance, side effects and quality-of-life scores. Patients in both groups were demographically similar, and had comparable levels of preoperative pain.
As Dr. Estebe reported at the 2013 annual meeting of the American Society of Anesthesiologists (abstract 2067), patients in the study group demonstrated a trend of decreasing pain at rest in the seven days before surgery (P=0.144), which became significant thereafter (P=0.022). The French team found a trend toward decreased postoperative pain with motion in these patients, but it did not reach statistical significance (P=0.128).
The effect of the low-polyamine diet became significant when the investigators analyzed the subset of patients experiencing more severe pain at rest and with motion (P=0.0135 and 0.0093, respectively). No reduction in pain was observed in controls.
Quality-of-life scores were significantly improved in the low-polyamine diet patients immediately before surgery (P=0.046), and continued as a trend five days after surgery (P=0.0629). Hospital length of stay was similar for both groups of patients.
“In terms of compliance, it’s very interesting to note that 100% of the study group completed the diet for the seven days before surgery, compared with 83% thereafter,” Dr. Estebe said. “By comparison, 83% and 71% of controls consumed both drinks each day before and after surgery, respectively. The only side effect was minor gastrointestinal intolerance. So a low-polyamine diet could be useful for surgery because pain is decreased, compliance is high and adverse effects show no difference between the two groups.”
Eugene R. Viscusi, MD, professor of anesthesiology and director of acute pain management at Thomas Jefferson University, in Philadelphia, called the study “fascinating.”
“Some diets can promote inflammation, which might have a role in pain. Here, the authors identified another familiar pathway involving the NMDA receptor, which is well known to have a role in chronic pain, particularly in the presence of chronic opioid use. There is a resurgence of interest in ketamine—a potent NMDA receptor antagonist—in patients with opioid tolerance, and this drug is now commonly used in this setting. So it is entirely possible that modulation of diet in a way that modulates the NMDA receptor might have an effect on pain.”
Yet Dr. Viscusi raised several questions about the study. “The experimental group not only had polyamine restriction but also received what appears to be a markedly different caloric load during the study,” he said. “One has to question whether this alone, or perhaps the type of calories, made the difference.
“One thing is for sure: We generally do not pay close enough attention to the diets of our perioperative patients,” Dr. Viscusi added. “Perhaps careful preoperative and postoperative feeding may have a far greater impact than we ever imagined.”
It has been estimated that 1 in 4 people in the US suffer from some form of chronic pain in their lifetime. The duration of this pain differs from person to person, spanning several weeks to many years.
Many sufferers of long-term chronic pain can have their daily wellbeing severely affected if treatments fail to offer appropriate levels of pain relief.
Of the more than 1.5 billion people worldwide said to suffer from chronic pain, the most common area affected is the lower back. The frequency of this is 23-26% of the global population.
Not surprisingly, this has been a hot area of research, which has produced treatment options from opioids to surgery. Opioids, while very effective for analgesia, can produce unwanted long term problems like dependence for chronic pain patients.
For this reason, surgical options are frequently presented for long term chonic pain patients. One such technique is spinal cord stimulation therapy (SCS), where pulses are delivered to the spinal cord by a small device implanted under the skin, emitting a form of paresthesia. As many as 50,000 patients in the US undergo SCS ever year to combat chronic pain.
Paresthesia is a sensation akin to tingling and is a result of SCS. When a device is turned on, an electrical current interrupts the pain signal being sent to the brain. Although a patient’s pain is not cured, SCS hopes to offer some temporarily relief.
Although SCS has been shown to reduce pain, many patients find the paresthesia that accompanies this to be uncomfortable.
This was to be the catalyst for scientists to develop a new form of SCS, one which still alleviates pain but reduces the effects of paresthesia in patients.
Traditional SCS uses frequencies of 40-60 hertz. Scientists decided to intensify this and use high-frequency pulses capable of delivering up to 10,000 hertzes. The new treatment has been named HF10.
Prof. Leonardo Kapural, lead study author and professor of anesthesiology at Wake Forest University School of Medicine and clinical director at Carolinas Pain Institute at Brookstown in Winston-Salem – both in North Carolina – believes the research to be the first of its kind.
“This is the first long-term study to compare the safety and effectiveness of high-frequency and traditional SCS therapy for back and leg pain,” he explains.
Scientists examined 171 patients with chronic back or leg pain, of whom 90 received HF10 therapy and 81 were treated with traditional SCS.
After 3 months, researchers found 85% of back pain and 83% of leg patients receiving HF10 therapy reported a 50% reduction in pain or greater. These patients also reported no experience of paresthesia.
In contrast, patients undergoing SCS reported less effective results. Only 44% of back pain patients and 56% leg patients experienced a minimum 50% reduction in pain.
The study ran over a 12-month period and found HF10 to be more effective compared with traditional SCS. More than half of the HF10 sample group reported being “very satisfied” with the outcome, compared with just 32% of patients who received traditional SCS.
Prof. Kapural hopes this research will be an important step toward treating chronic pain.
SCS represents an alternative for those patients who wish to avoid surgery or drugs such as opioids. According to a 2011 report, at least 100 million adult Americans suffer from chronic pain. In the same report, it was also estimated that chronic pain costs society between $500-635 billion a year.
Dr. Hanna has many years of experience performing SCS procedures for chronic pain patients. To learn if this procedure might be right for you, please make an appointment with Dr. Hanna at the Florida Spine Institute in Clearwater, FL. His contact information can be found here.